Are you currently pregnant and wondering if your pelvis is wide enough for a vaginal delivery?
Were you told you would need to have a cesarean section because of “CPD?”
Don’t worry, you are not alone!
After reading this post, you’re going to learn:
- the four different types of pelvises,
- how to know which shape pelvis you have, and
- how to know if you will be able to have a vaginal delivery based on the type of pelvis you have.
Let’s get started.
The 4 Types of Pelvic Shapes
There are four different types of pelvic shapes you can have.
They are:
- Gynecoid
- Android
- Anthropoid
- Platypelloid
Gynecoid
The gynecoid pelvis is the most common pelvis shape in women. One study found that approximately 51% of women have this shape.
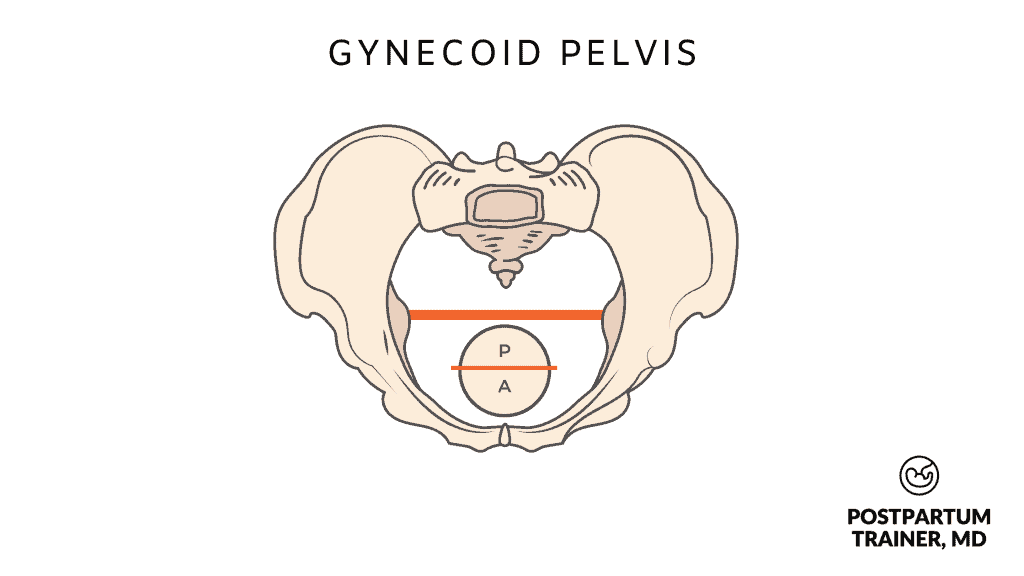
It is round and wide to accommodate a baby.
This pelvic type is also most common in Caucasian women.
Android
The android pelvis resembles the male pelvis more so than a female pelvis. It is narrower anteriorly and shaped like a heart.
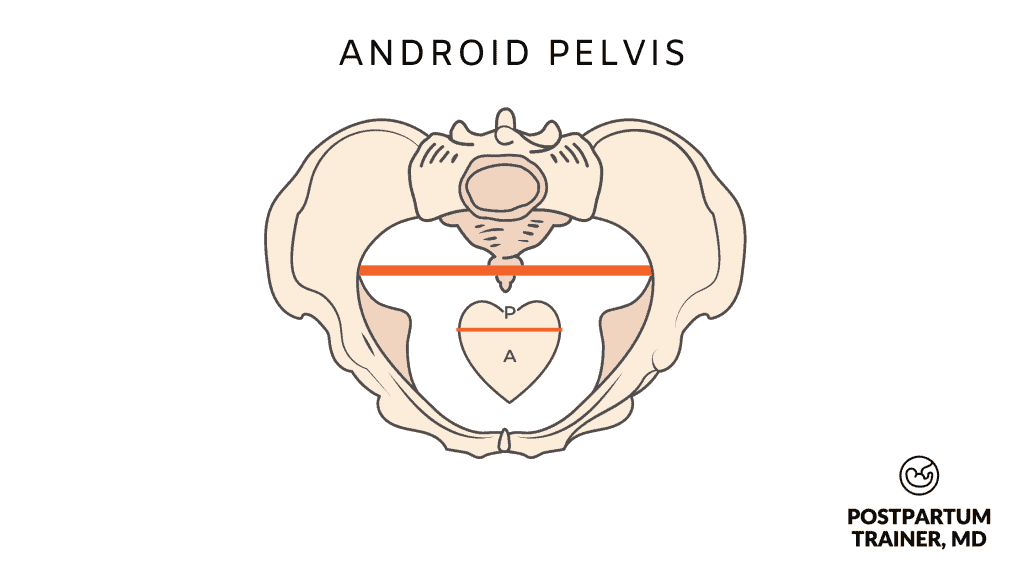
Women with an android pelvis may have difficult and long labors as the baby tends to move slowly down the birth canal.
Anthropoid
The anthropoid pelvis is also a narrow pelvis compared to the gynecoid pelvis- and it resembles an oval.
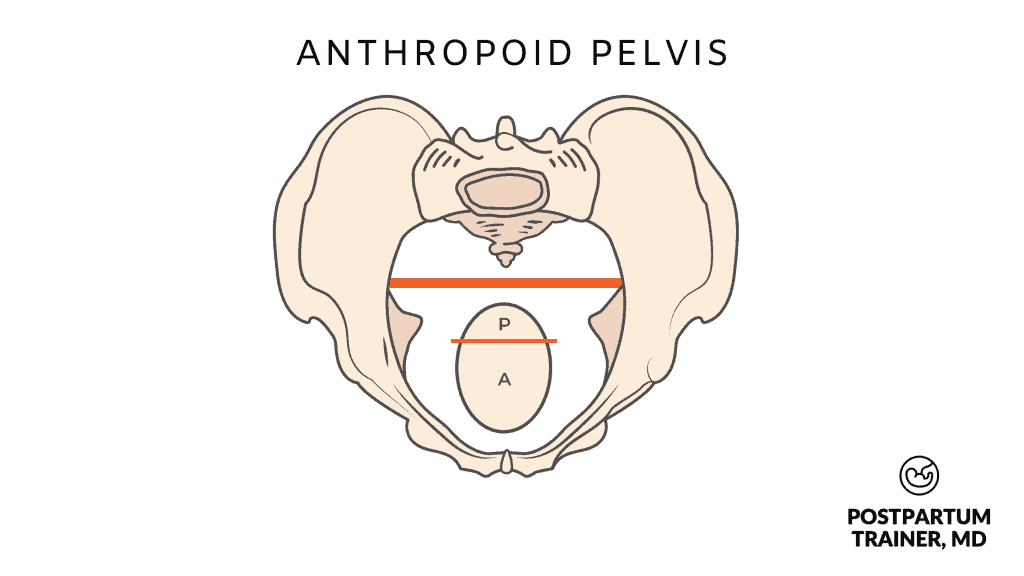
This pelvic shape is common in African women and can cause long labors due to the position of the baby.
The anthropoid pelvis tends to keep the baby in an occiput posterior position. This means that the baby is looking up toward the ceiling.
This position is harder to deliver, as the baby would have to extend its neck to come out, rather than flex its neck.
Platypelloid
Lastly, the platypelloid pelvis is the least common type of pelvis. It is flat and also makes vaginal delivery more difficult.
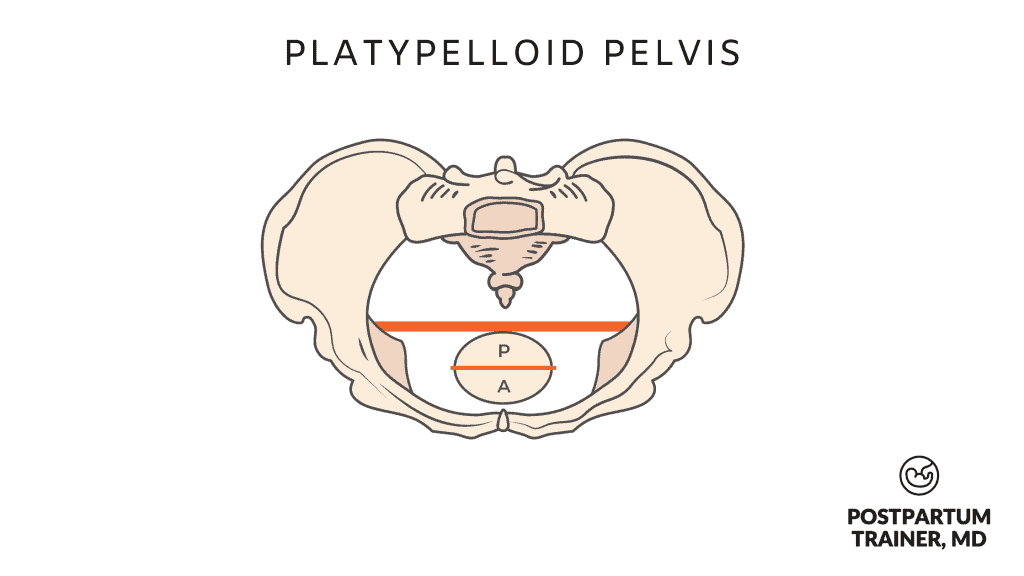
Given the oblong shape of the pelvis- it is also associated with fetal positional changes.
Platypelloid pelvises are associated with a persistent occiput transverse position in which the baby is looking left or right.
This position is not ideal for vaginal delivery.
Many women with this type of pelvis may need a cesarean delivery.
How do I know what shape my pelvis is?
The only way to determine the shape of your pelvic bone is to do some type of radiographic imaging study.
This can be done with an x-ray or a 3D CT scan.
Many years ago, physicians would actually have their patients get an x-ray to see if their pelvis was adequate.
This is no longer recommended- especially not for a pregnant woman.
Unfortunately, a physical exam is not a reliable way of determining which of the four pelvic types you have.
Is it harder to give birth with small hips?
If you have small or narrow hips it can definitely be harder to give birth vaginally.
The reason is that your baby will have a hard time passing through the birth canal.
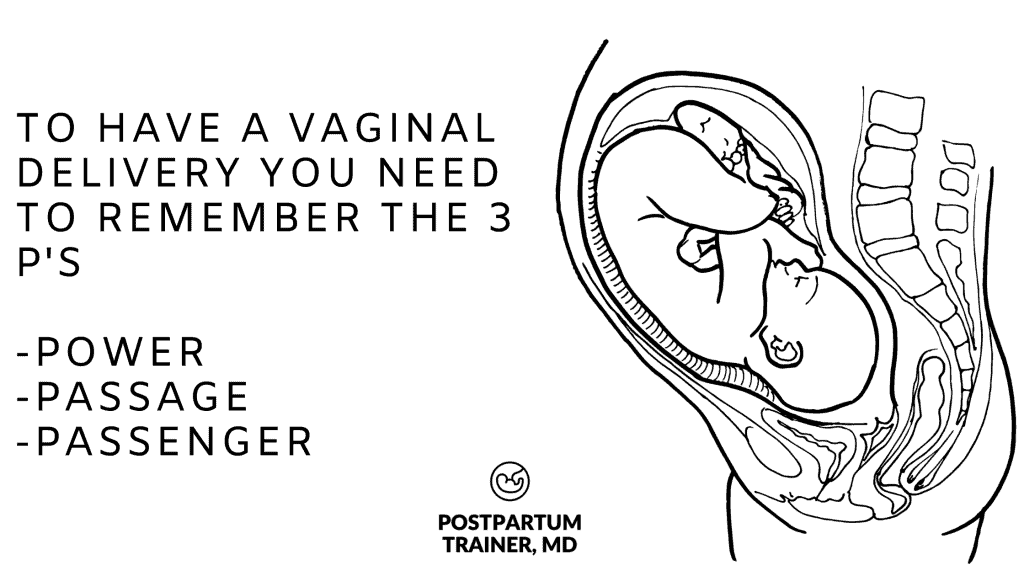
In order to have a vaginal delivery you must think of the 3 P’s.
- Power
- Passage
- Passenger
The first P is power.
Power refers to the strength of the uterine contraction.
If you are not having adequate, strong uterine contractions, your baby will not move down the birth canal.
The second P is passage.
If the passage or pelvis is too narrow, this will obstruct your baby from coming down or take a really long time to come out.
Also, if you have a pelvis other than gynecoid – it will be harder to deliver vaginally.
The third P is passenger.
The passenger refers to your baby.
If your baby is considered macrosomic or large for gestational age, and you have a small pelvis, the baby might not be able to fit.
If your baby is not in the correct position, it will also take a long time to pass the birth canal and deliver.
How do you know if a baby will fit through the pelvis?
Usually, at your first prenatal visit, your physician will perform a pelvic exam and make some rough measurements.
The first thing we try and determine is something called the diagonal conjugate.
The diagonal conjugate is the measurement from your pubic symphysis, aka the pubic bone, to your sacral promontory, aka the tail bone.
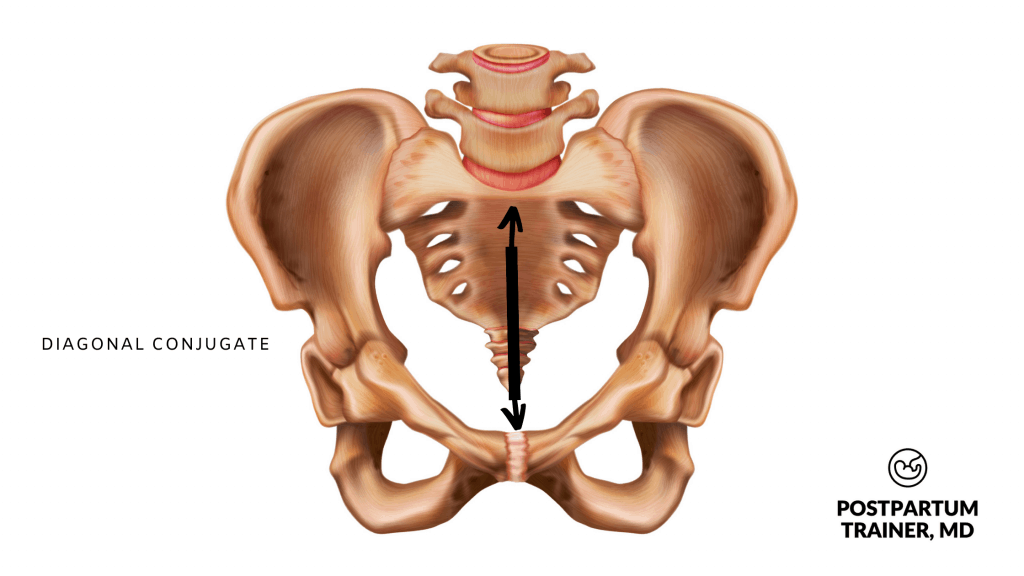
Ideally, this distance should be roughly 11-12 cm.
Assuming that a baby’s head is ~10cm, a baby should fit through the pelvic outlet if the diagonal conjugate is 11-12cm.
(It’s a different story if you have gestational diabetes as your baby’s shoulders may be even wider, putting you at risk of shoulder dystocia. This is when the head delivers, but the shoulders don’t.)
When you are getting close to delivery, your physician will also determine if your baby will be able to fit with one other method.
They will use an estimated fetal weight of you baby and compare that to the size of your pelvis.
If your baby is estimated to be 5kg or more, a c-section will be recommended.
How can I widen or increase my pelvic size for birth?
Unfortunately, there is no proven way to widen or increase your pelvic size for childbirth.
Luckily for all of us, our bodies are extremely smart and can adapt to changes that occur to it.
During pregnancy, your body will begin to release a hormone known as relaxin.
This hormone does exactly what the name implies.
It begins to relax the ligaments and joints surrounding your pelvis so that your hips can open up a bit more to accommodate your baby.
So just relax and let your body do its thing!
What happens if your pelvis is too small to give birth?
You may be wondering – can you be too small to give birth naturally?
Unfortunately, it is possible to be too small to give birth naturally.
This is called cephalopelvic disproportion or CPD for short.
We use this term when we deem that your pelvis is too small to deliver your baby vaginally.
Often, this is the case when the baby has a high estimated fetal weight and the mom is petite.
If your physician believes this to be the case, you will be offered a cesarean section.
How To Minimize The Risk of CPD
So what should you do to minimize the risk of your baby not fitting through your pelvis?
The biggest thing you should do is to try and stick to the recommended weight gain guidelines during pregnancy. This will minimize your risk of developing a large infant.
In addition, be sure to get screened for gestational diabetes in the third trimester.
If you are diagnosed with GDM, keep your blood sugars under control through proper nutrition and follow very closely with your obstetrician.
The key is to try and keep your estimated fetal weight in a healthy range.
Related Questions
Do hips get wider after birth?
Your hips can get wider after birth due to the hormone relaxin that was released throughout your pregnancy.
This hormone was released in an effort to loosen the ligaments and joints in your pelvis allowing your pelvis to open up a bit more.
Another reason hips can get wider after birth is if you have something called pubis symphysis diastasis aka pelvic girdle pain.
This is a medical condition in which there is a pathologic separation in your pubic bone after a vaginal delivery.
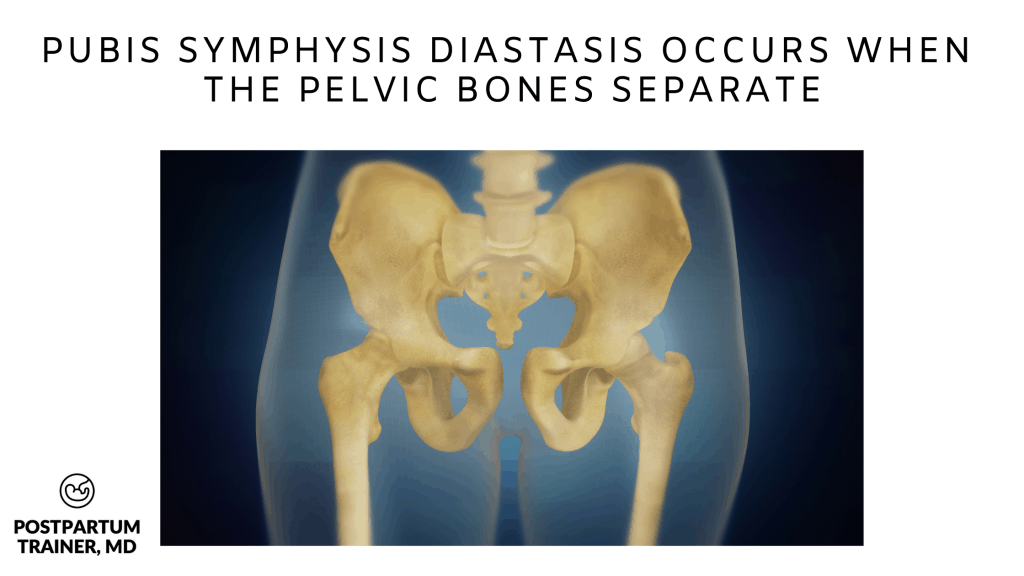
Typically women have severe pelvic pain with any sort of movement postpartum.
If you believe you have this condition, please check out my post on How To Get Relief From Symphysis Pubis Dysfunction to learn more about what you could do.
Can a short woman give birth naturally?
Short women can give birth naturally as long as their pelvis is adequate, and their baby is proportional in size.
Maternal height becomes an issue if the male partner is much larger than the woman.
I often see petite women who are 5 feet tall and weigh 100 lbs with partners who are over 6 feet and 200 lbs.
This is a recipe for having an infant that is too large for you and CPD.
Is a small pelvis hereditary?
It is reasonable to assume that having a small pelvis is hereditary.
Athletic parents tend to have athletic children.
Larger parents tend to have larger babies. So if your mother’s pelvis is small, it is likely that you have a small pelvis too.
Final Words on Small Pelvis and Pregnancy
Are you curious to know what type of pelvis you have?
It is likely you have an adequate pelvis if your doctor has not mentioned a concern about your pelvis to you before.
Try not to focus too much on your pelvis type as there are:
- plenty of women who have a “normal” pelvis and end up with a cesarean section for other reasons, and
- plenty of women with a small pelvis who have a vaginal birth.
Just focus on doing your best to have a healthy pregnancy and a healthy baby.
Now I want to hear from you.
Were you ever told you had a small pelvis?
Did you have a successful vaginal delivery?
Comment below and let me know.
Get Four Free Workouts To Help Strengthen Your Pelvic Floor & Heal Your Mommy Tummy!

Brittany Robles, MD, MPH, CPT
Brittany Robles is a full-time OBGYN physician, a NASM certified trainer, and a prenatal and postnatal fitness specialist. She holds a Master of Public Health degree in maternal health with a special interest in exercise and nutrition. She is also the co-author of The White Coat Trainer. Learn more about her here.
Sharing is Caring – Send This To A Mom In Need!
Other Related Articles
- How To Gain Minimal Weight While Pregnant
- The Belly Only Pregnancy – Is It Possible [Or Healthy?]
- 10 Exercises To Help You Prepare For Labor
References:
- Salk I, Cetin M, Salk S, Cetin A. Determining the Incidence of Gynecoid Pelvis Using Three-Dimensional Computed Tomography in Nonpregnant Multiparous Women. Med Princ Pract. 2016;25(1):40-48. doi:10.1159/000440808
- MacLennan AH. The role of the hormone relaxin in human reproduction and pelvic girdle relaxation. Scand J Rheumatol Suppl. 1991;88:7-15. PMID: 2011710.
From what I have read and researched, true cases of CPD are very rare. I have a hard time believing that 49% of women have anatomies that make delivering a baby difficult. I also have a hard time believing that women who are not Caucasian will also have difficulty delivering a baby because of their anatomy. In America, the medical model of birth has women numbed and lying on their backs to deliver. This makes delivery difficult for even the most “ideal” anatomy (whatever that might mean). Looking at documents of indigenous women throughout the world, they did not give birth like we do in our hospitals. They stood, squatted, side-lay, got on all fours, etc. We do not see them lying stationary on their backs. So it might not be the pelvis shape that causes problems but the entire model to which we subject birthing women in America. In physiologic labor and birth, the woman’s position plays a vital role in the mother’s ability to accommodate baby. I have heard stories of mothers who were told they had CPD only to deliver their babies vaginally and unmedicated. Birthing position has been greatly undervalued in the medical model of birth. Discussing the evidence behind birth positions allowing for increased pelvic width so the baby can make his way through the birth canal would be a good perspective to add to your post. Also, focusing on the fact that our bodies are made for birth could help your readers and patients begin to trust what their bodies can do. Empowering women to strength train and stay fit, as you do, shows one way we can better harness our bodies’ innate abilities. But also, through understanding our bodies’ roles in labor and birth, we can be empowered. Instead of bringing up questions that raise doubts in women’s minds about their abilities to successfully vaginally birth their babies, looking at the evidence and statistics might give women a more positive impression of what they can achieve.
Here are some articles I found explaining some of what I have gleaned through my years of informal research:
https://www.bellybelly.com.au/birth/small-pelvis-big-baby-cpd/
https://www.thevbaclink.com/your-pelvis-is-not-too-small/
Hi Erica,
Thank you so much for your comment. You bring up very interesting points.
Although lying on your back is the standard birthing position in America, providers are often open to delivering babies from various positions. I have personally delivered babies from a side-lying position as well as all fours.
I agree with you that empowering women to understand their bodies and role in labor and birth is super important and it is something I do throughout the prenatal care.
At the end of the day, our goal as obstetricians is to have a healthy mom and healthy baby. Unfortunately we see a ton of macrosomic infants and vaginal delivery is not for everyone.
We will always elect for a cesarean section to ensure maternal and fetal wellbeing in order to prevent irreversible damage to the mom or baby i.e a really bad postpartum hemorrhage resulting in a cesarean hysterectomy or cerebral palsy and/or nerve damage from a shoulder dystocia.
I am in 39weeks of pregrancy, but my baby head is not fixed.BPD of my baby is 9.54cms.Is this the reason still my baby position is not fixed?
My gynec is suggesting for c-section.
Please let me know should I wait till my completion of 40 weeks?
Hi Mounika,
Thank you so much for your comment.
Unfortunately I cannot give you personalized medical advice.
I would go with the recommendation of your obstetrician as he/she knows you and your current situation best.
I gave birth via C.S after a long labour i was later told that i had a nareow pelvics.